What is external cephalic version?
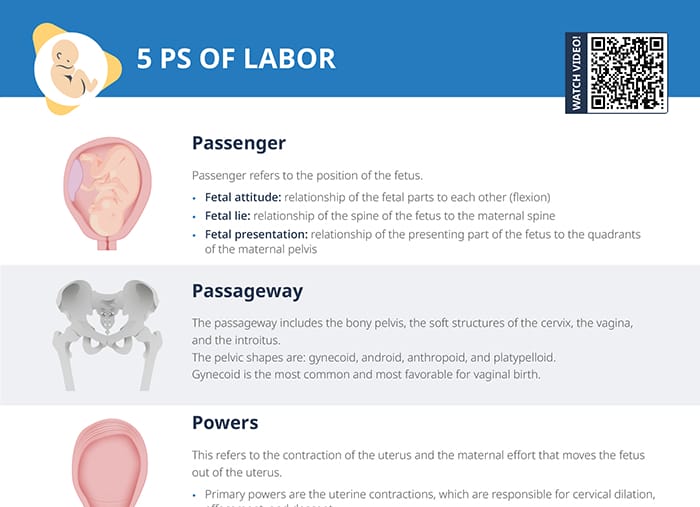
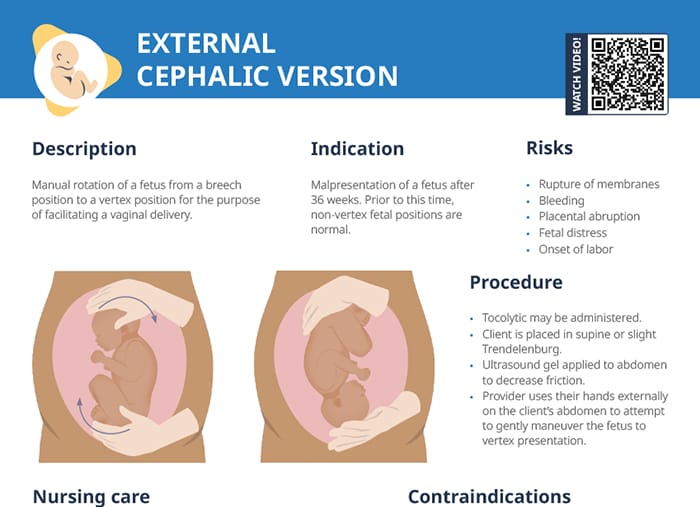
External cephalic version refers to a procedure to manually rotate a fetus from a breech position to a vertex position. Vertex position facilitates vaginal delivery.
Indications
External cephalic version is indicated if a fetus is malpresenting after 36 weeks. Prior to this time, non-vertex fetal positions are normal.
Success rate
External cephalic version is successful approximately 50% of the time.
Related videos
Risks and contraindications
Contraindications
ECV should not be performed if any the following is present:
- Placenta previa
- Client has had a classical C-section before
- Ruptured membranes
- Low amniotic fluid levels
- Non-reassuring fetal monitoring
- Multiple gestation
Risks
Manually rotating a fetus causes a risk of:
- Rupture of membranes
- Bleeding
- Placental abruption
- Fetal distress
- Onset of labor
ECV procedure: steps and nursing tasks
Nursing care
- Ensure consent forms are signed.
- Obtain baseline nonstress test.
- Ultrasound may be performed.
- Confirm RhoGAM was given at 28 weeks for Rh-negative clients.
- Administer IV fluids and tocolytics as ordered.
- Monitor the fetus after the procedure.
Procedure
A tocolytic may be administered, and an ultrasound gel is applied to the abdomen to decrease friction. The client is placed in supine or slight Trendelenburg position.
The provider uses their hands externally on the client’s abdomen to attempt to gently maneuver the fetus into a vertex position.
After a successful procedure, labor may be induced to decrease the chance of the fetus changing position again.
Internal cephalic version
Internal cephalic version is a more invasive way of repositioning the fetus, with the provider reaching a hand up through the cervix and manually turning the baby there. It is performed less commonly and reserved for specific circumstances.
Client care and education
Make sure to educate clients to notify a provider if:
- Vaginal bleeding occurs
- Their water breaks
- Contractions start
- They notice a decrease in fetal movements
Some clients experience mild discomfort during the procedure, while others do find it painful. Provide reassurance and check if pain relief options are warranted.
Since an external cephalic version is only successful in half the cases, make sure to manage client expectations before the procedure and explain why an attempt may be recommended anyway in the specific case.