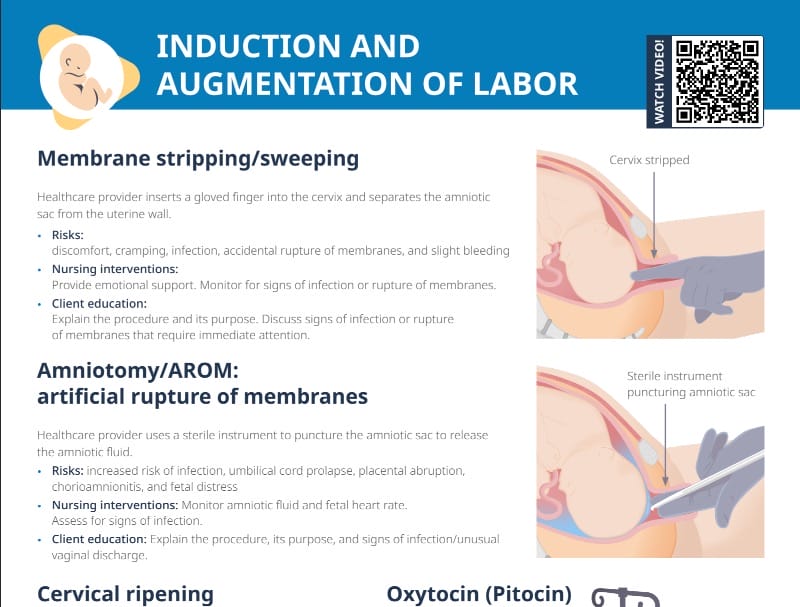
What is amniotomy or the artificial rupture of membranes (AROM)?
Amniotomy is a procedure where the amniotic sac that surrounds the fetus is intentionally ruptured by a provider. Therefore, amniotomy is also called the “artificial rupture of membranes” or “AROM.”
This procedure is often performed as part of the labor management process.
Indications and contraindications for amniotomy
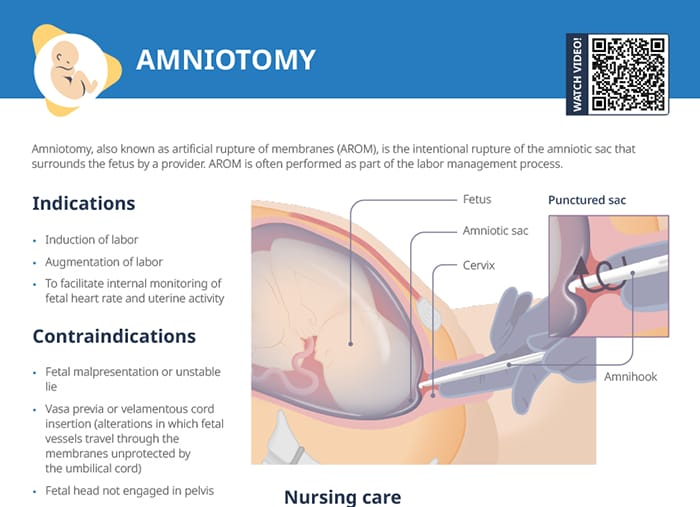
Indications
Amniotomy is indicated in the contexts of induction of augmentation of labor, as well as to facilitate internal monitoring of fetal heart rate and uterine activity.
Contraindications
- Fetal malpresentation
- Unstable fetal lie
- Vasa previa
- Velamentous cord insertion
- Fetal head not being engaged in the pelvis
Risks that come with the artificial rupture of membranes
Cord prolapse and infection are the biggest risks that come with artificially rupturing the amniotic sac.
When the amniotic sac is ruptured, the buoyancy within it is removed and the fetus descends. If the umbilical cord is floating below a disengaged fetal head when this occurs, cord compression will result in fetal hypoxia and necessitate emergent cesarean delivery.
Breaking the protective barrier around the fetus increases the risk of chorioamnionitis, particularly if AROM is performed early in labor.
Amniotomy procedure: steps and nursing interventions
Nursing care before an amniotomy
Before an amniotomy is performed, ensure the client has consented and received an explanation of the procedure. The client and their family should have all their questions answered.
Assess and document the client’s vital signs and the fetal heart tones, as well as the fetal station. Gather the supplies:
- Sterile gloves, sterile gauze and swabs, antiseptic solution, sterile drapes, underpads for the bed
- Amniotic hook
- Fetal heart rate monitor
- Documentation supplies and emergency supplies including oxytocin in case contractions need to be strengthened
An amniotomy hook, amniotic hook, or “amnihook” is the instrument used to rupture the membranes. It is a long plastic device with a small hook at the end.
Procedure steps
The procedure is done by a provider with the assistance of a nurse. The procedure steps after preparation are as follows:
- Inserting a speculum into the vagina to visualize the cervix; then inserting the amniotic hook through the cervix to reach the amniotic sac
- Using the hook to carefully tear the membrane
- Assessing the amniotic fluid flowing out (e.g. for meconium staining or infection)
During the procedure, important nursing tasks include assisting the client into the correct position, assisting the provider with supplies, and reassuring the client.
Post-procedure tasks
- Fetal heart tones should be assessed immediately following amniotomy.
- Also assess the color and odor of the amniotic fluid.
- Assist the client with a dry gown and linens as needed.
- The contractions following the amniotomy may be intense, so make sure to offer emotional support and reassurance to the client during the subsequent labor process.
Client questions and education
After the water breaks, how long can the baby survive?
Reassure your client that the baby is being closely monitored and labor is expected to progress after the membranes are artificially ruptured. How long the baby is safe in the uterus after the membranes have ruptured depends on many factors.
What happens if the water breaks too early?
A premature rupture of membranes (before the onset of labor) is recognized by painless discharge of clear or yellowish fluid, either as a large gush or as intermittent trickles. Management depends on how far the pregnancy has progressed: After 34 weeks, labor will be induced. If earlier, measures will be taken to prolong the pregnancy as much as possible to give the fetus the maximum possible time to mature.
If the water breaks and the time until the onset of labor extends beyond 18 or 24 hours, the condition is called prolonged rupture of membranes. This increases the infection risk, so labor will likely be induced and measures against infection will be taken.
What does it look like when your water breaks?
The water can be discharged from the vagina in a sudden gush, or in a slower intermittent trickle (sometimes mistaken by clients for urine). Typically happening during labor, it may occur before labor starts (premature rupture of membranes).
The fluid should be clear or slightly yellowish with a mild odor; colors like green, brown, and foul odors can indicate problems like infections or meconium staining.